Walmart’s Mega Nudging Test
Walmart partnered with academics whose listing on the published paper reads like the credits on a Hollywood blockbuster movie, which is to say almost as long as the movie.
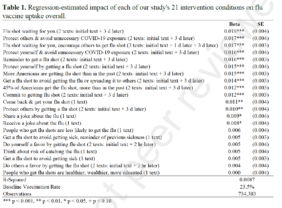
The aim? Increasing flu vaccination rates in hopes it would provide guidance for increasing Covid vaccine uptake.
This team of social scientists came up with 22 evidence-based messages to boost vaccination rates. The nudge messages were texted to over 700,000 Walmart pharmacy patients last fall and encouraged folks to visit Walmart for a flu vaccine.
There are reams of lessons to be learned for anyone whose job it is to get another human being to do something – i.e. everyone reading this.
The scientists banded together in small teams to devise their different communication strategies relying, as you’d imagine, on theory and evidence to guide their “ideation”.
Lesson One: No blue-sky here. The best innovation comes from understanding, not inspiration or divine intervention.
Lesson Two: Small teams of experts are always better than ‘consensus’ teams of non-experts or hierarchical teams where biggest title opinions win out, or death by committee review.
The messages ranged from interactive (i.e. requesting replies) to informational, some included just one message, others had follow-up texts sent up to three days later.
Each team had their study design, analytical and predicted outcomes preregistered.
Lesson Three: If you don’t specifically state what the outcome of your test will be and why, it’s almost certainly random guessing and should never have donor dollars spent on it.
Lesson Four: If you don’t have an analytical plan to determine if the test won or lost then don’t spend donor dollars testing it. Note: this plan should be more rigorous than eyeballing percentages and ideally more than running a simple bivariate, statistical test. Most of the analysis in the Walmart testing used regression that allows for control variables – e.g. patient age, race/ethnicity, gender.
The teams decided to focus on the population who is not opposed to the flu vaccine rather than the skeptics. They did this by selecting patients who had received the flu shot the prior year. All the messaging was therefore aimed at closing the intention-action gap where we lack sufficient motivation to do what we intend to do.
Lesson Five: People are different. One-size-fits-all is never optimum. Our critique of this work is that it still doesn’t go far enough in getting beyond one-size-fits-all. They did what most do, use what’s available and convenient (e.g. data on who got the shot last year) rather than force themselves to dig deeper into how this population could be further subdivided based on Identity or Personality, for example.
We’ve listed the 22 interventions rank ordered by effectiveness. The top performing message told folks there was a flu shot waiting for them. This is based on the endowment principle and loss aversion. The shot belongs to me. “I don’t want to give it up” because we are much more averse to loss than seeking gain (even if the two are equal). There is likely a sense of reciprocity as you’ve taken the time to set this aside for me, it would rude be or impolite to not take it.
The messages that were more clever or informal – sharing a joke – were less effective
Lesson Six: Context is king. This is a pharmacy as messenger. That invokes a level of formality and seriousness. The tone that matched expectation and situational norms worked best.
“Best practice” is not the winning message, envelope or sequence. It is the process.
 Kevin
Kevin
Behavioral Science Q & A
Thanks so much for raising this. Yes, capturing donor information can be helpful for stewardship like newsletters, thank-you letters, impact updates. But how you ask matters. Forcing full data capture introduces friction that can significantly depress conversion, many donors may simply abandon the process. Beyond the friction itself, required fields also shift the emotional experience […]
Read Full Answer
Unlike holidays that everyone already knows, Giving Tuesday is a created event. Many donors recognize the name but not the exact timing, so referencing it becomes a helpful cue. It serves as a reminder and taps into social norm activation (“everyone’s giving today”), which boosts response. However, we still want it paired with the mission, […]
Read Full Answer
When a subject line leads with the match (“Your gift matched!”), it risks triggering market-norm thinking: the sense that giving is a financial transaction rather than an act rooted in values, identity, and care. This shift reduces intrinsic motivation and, over time, can weaken donor satisfaction and long-term engagement. It also makes the email indistinguishable […]
Read Full Answer
There’s no evidence that QR codes suppress mid-value giving; all available research suggests they either help or have no negative effect. In fact, behavioral and usability research consistently shows the opposite: reducing friction at any point in the donation process increases completion rates and total response. And that has nothing to do with capacity and […]
Read Full Answer
What you’re experiencing is very common. Resistance often isn’t about capability, but about motivation quality. If board members feel pushed into fundraising, that triggers controlled motivation (low quality motivation) i.e. obligation, guilt, or fear of judgment, which often results in avoidance. Instead, we need to create conditions for volitional motivation (high quality motivation) by satisfying […]
Read Full Answer
That’s a really thoughtful question, and you’re not the first to raise it. Many of our clients have been cautious about placing the ask at the very end. To address their concern, we’ve tested both approaches, and the results are clear: when the ask comes last, even if that means it appears on the second […]
Read Full Answer